PARAGANGLIOMA
Paragangliomas refer to abnormal cell growths that form a specific type of nerve cell found throughout the body. Such specific nerve cells (chromaffin cells) perform significant functions in the body, including the regulation of blood pressure. When chromaffin cells transform into abnormal cells, these cells can form tumors. In other words, a paraganglioma refers to a rare neuroendocrine (catecholamine secreting) neoplasm that may develop at various sites in the body (such as the head, neck, thorax and abdomen).
Location of this type of tumor in the adrenal gland changes its term to a pheochromocytoma (also called intra-adrenal paraganglioma). These involve rare tumors, with an overall estimated incidence of 1 in 300,000. No test determines the benign from the malignant tumors, therefore, oncologists recommend long-term follow-up for all individuals with paraganglioma. Specific locations of this tumor include the jugular foramen, ear, and adrenal medulla, pre-aortic and parasympathetic plexuses.
Other names for paranganglioma include: chemodectoma, carotid body tumor and glomus cell tumor.
Signs and symptoms of Paraganglioma
Most paragagliomas present as a painless and asymptomatic mass, or create symptoms such as;
- Hypertension
- Tachycardia
- Headache
- Palpitations
- Profuse sweating
Although all paragangliomas contain neurosecretory granules, only in 1-3% of cases can excess secretion of hormones such as catecholamines have clinical significance, in that case, manifestations often resemble those of pheochromocytomas (intra-medullary paraganglioma).
Sites of Origin
About 85% of paragangliomas develop in the abdomen; only 12% develop in the chest and 3% in the head and neck region (the latter most likely present as symptomatic). One can describe paragangliomas by their site of origin and special names which aid description:
- Head and neck paraganglioma (HNPGL)
Various types of paraganglioma occur in the head and neck, most may have specialized names depending on the precise location.
- Carotid paraganglioma (carotid body tumor)
This refers to the most common of the head and neck paragangliomas. It usually presents as a painless neck mass but larger tumors may cause cranial nerve palsies, usually of the vagus nerve (CNX) and hypoglossal nerve (CNXII).
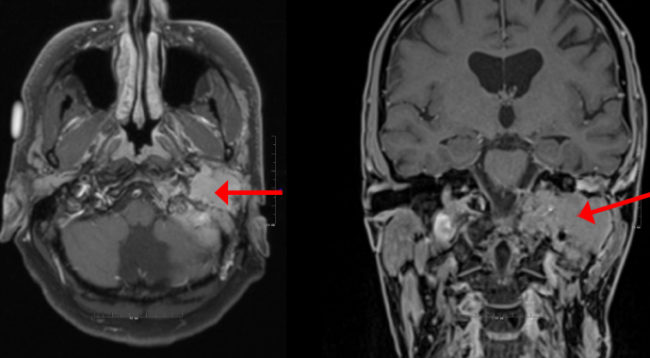
- Glomus tympanicum and Glomus jugulare:
These tumors also commonly refer to as jugulotympanic paraganglioma. Both tumors commonly present as middle ear mass resulting in tinnitus (in 85%) and loss of hearing (in 65%). The tumors may compress the cranial nerves of the jugular foramen, resulting in swallowing difficulty, or ipsilateral weakness of the superior trapezius and sternocleidomastoid muscles (from compression of the spinal accessory nerve, CNIX). These patients present with an inflammation behind an intact ear drum. This condition also identifies as the “Red drum”. On applying pressure to the external ear canal with the help of a pneumatic ear speculum, whitening of the mass occurs. This sign refers to as “Brown’s sign”. A deficient bony plate along the tympanic portion of the internal carotid artery involves a normal variant. One can mistake this variant with the glomus jugulare.
- Pulmonary paraganglioma
These tumors occur in the lungs and may have either single or multiple sites. Pulmonary paraganglioma may manifest as an asymptomatic chest mass with radiological characteristics of benign tumors.
- Organ of Zuckerkandl
This refers to a collection of paraganglia located near the bifurcation of the aorta, comprising a small mass of neural crest-derived chromaffin cells. This serves as a common origin of abdominal paragangliomas.
- Vagal paraganglioma
This refers to the least common of the head and neck paragangliomas. These tumors usually present as a painless neck mass, but may result in dysphagia and hoarseness.
- Other sites
Uncommon sites of involvement include the larynx, nasal cavity, paranasal sinuses, thyroid gland and the thoracic inlet, as well as the bladder in extremely rare cases.
Diagnosis
Accordingly, paragangliomas fall into categories as originating from a neural cell line in the World Health Organization classification of neuroendocrine tumors. Given the fact that paragangliomas originate from cells of the orthosympathetic system, these tumors closely relate to pheochromocytomas; chromaffin-positive tumors.
Treatment
The main treatment for paraganglioma includes surgery, embolization and radiotherapy.
References
- “Pheochromocytoma and Paraganglioma Treatment (PDQ) -Patient Version- NCI”. www.cancer.gov December 23, 2011.