LP SHUNTS
What’s an LP shunt?
A shunt refers to a tube, catheter or “surgically created anastomosis” designed to bypass or redirect body fluids from one point in the body to another. Specialists use lumbar-peritoneal shunts in neurological disorders, in cases of chronic increased intracranial pressure to drain excess cerebrospinal fluid (CSF) from the subarachnoid cisterns associated with certain health conditions such as hydrocephalus and benign intracranial hypertension (BIH), also known as idiopathic intracranial hypertension (IIH) and pseudotumor cerebri (PTC). The more preferred name for this condition includes idiopathic intracranial hypertension (IIH).
Medical shunts fall under various categories, but specialists make use of two main categories in treatment of chronic increased intracranial pressure due to cerebrospinal fluid (CSF). These include the cerebral shunts and the lumbar shunts (extracranial shunts). Various types of shunts within these two categories include:
Cerebral shunts
- Ventriculo-pleural shunt (VPL shunt)
- Ventriculo-peritoneal shunt (VP shunt)
- Ventriculo-atrial shunt (VPL shunt)
Lumbar shunts
- Lumbar-peritoneal shunt (LP shunt)
- Lumbar subcutaneous shunt (LS shunt)
Lumbar-peritoneal (LP) Shunt
A lumbar peritoneal (LP) shunt refers to a technique of cerebrospinal fluid (CSF) diversion from the lumbar thecal sac to the peritoneal cavity. It proves useful under a large number of conditions such as communicating hydrocephalus, idiopathic intracranial hypertension, normal pressure hydrocephalus, spinal and cranial CSF leaks, pseudomeningoceles, slit ventricle syndrome, growing skull fractures which prove difficult to treat by conventional methods(when dural defects deep in the cranial base or across venous sinuses and in recurrent cases after conventional surgery), raised intracranial pressure following chronic meningitis, persistent bulging of craniotomy site after operations for intracranial tumors or head trauma, syringomyelia and failed endoscopic third ventriculostomy with a patent stoma.
In spite of the large number of indications of this shunt and proving reasonably safe, good and effective, very few reports about the LP shunt presents itself in the literature. This procedure did not get its due importance due to some initial negative reports. This article aims to review indictations, complications, results and comparison of the LP shunt with the commonly practiced ventriculoperitoneal (VP) shunt.
Complications of an LP shunt
Common complications of LP shunt include:
- Shunt infection
- Malfunction (including dislocation, disconnection, migration, and obstruction)
- Arnold-Chiari I malformation (ACM)
- Subdural hematoma due to over drainage
- CSF leakage
- Radicular pain
Composition of LP Shunt
The lumbar peritoneal (LP) shunt composition and other types of shunts listed above may include a catheter or tube and various types of valves, although these shunts can just comprise of the tubing or catheter. Types of valves used in lumbar-peritoneal shunts (LP shunts) and cerebral shunts include the following:
- Sigma
- Anti-Siphon
- Delta
- Nulsen and Spitz
- Medium Pressure Cylindrical
The composition of a lumbar peritoneal shunt depends on the neurosurgeon performing the operation, no guidelines occur that determine what the composition of the lumbar peritoneal shunt should include for different types of cases. The composition of the lumbar peritoneal shunt can affect how well a patient will get on with the shunt and whether or not the patient may need revisions in the future, although specialists consider a number of other factors in whether or not a revision will prove necessary.
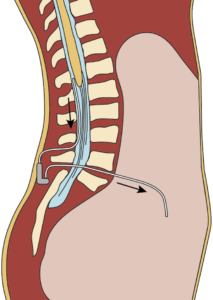
Placement
The surgeon inserts the lumbar-peritoneal shunt between two of the vertebrae in the lumbar region of the spine into the subarachnoid cavity, also known as the subarachnoid space.
The subarachnoid cavity refers to a spongy tissue-filled cavity that surrounds the brain and the spinal cord, this cavity contains the cerebrospinal fluid (CSF). The surgeon places the shunt under the skin and continues around the oblique muscles on one side of the body, and terminates at the peritoneal cavity, a cavity in the abdominal region of the body.
Once in place, the shunt drains the excess cerebrospinal fluid from the brain via the subarachnoid cavity and transports it to the peritoneal cavity, where its absorption occurs by the organs and passed out of the body during urination.
A lumbar subcutaneous shunt differs from these types of shunt in the cerebrospinal fluid that drains into the potential space immediately under the skin. The surgeon inserts a narrow tube into the subarachnoid space in the lumbar part of the back during a lumbar puncture. This tube then enters under the skin to a site where it can drain fluid, usually the flank.