STEREOTACTIC CRANIOTOMY
What’s a craniotomy?
A craniotomy refers to the surgical removal of part of the bone from the skull in order to expose the brain. This involves the use of specialized tools to remove the section of the bone called the bone flap. The surgeon temporarily removes the bone flap, and then replaces it after performing the brain surgery.
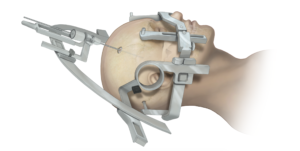
Stereotactic craniotomy refers to a type of craniotomy which involves the use of 3-dimensional imaging techniques such as magnetic resonance imaging (MRI) or computed tomography scan to surgically remove the section of the skull bone called the bone flap. This technique requires the use of a frame placed onto the skull or a frameless system using superficially placed markers or landmarks on the scalp.
Scans made of the brain, in conjunction with theses computers and localizing frames, provide a three-dimensional image, for example, a tumor within the brain. It proves useful in making the distinction between tumor tissue and healthy tissue and reaching the precise location of the abnormal tissue. Other uses include stereotactic biopsy of the brain (the surgeon guides a needle to an abnormal area to remove a piece of tissue for exam under a microscope), stereotactic aspiration (removal of fluid from abscesses, hematomas or cysts), and stereotactic radiosurgery (such as gamma knife radiosurgery).
Other types of Craniotomy
- Retro-Sigmoid “Keyhole” Craniotomy
Retro-sigmoid craniotomy (often referred to as “keyhole” craniotomy) refers to a minimally invasive surgical procedure performed to remove tumors. This procedure allows for the removal of the skull base tumors through a small incision behind the ear, providing access to the cerebellum and brainstem. Neurosurgeons may use this approach to reach certain tumors, such as meningiomas, acoustic neuromas (vestibular schwannomas), skull base tumors and metastatic brain tumors. Advantages of “keyhole” craniotomy include less pain after the procedure, quicker recovery, and less scarring.
- Translabyrinthine Craniotomy
Translabyrinthine craniotomy refers to a procedure that involves making an incision in the scalp behind the ear, then removing the mastoid bone and some of the internal ear (specifically, the semicircular canals which contain receptors for balance). The surgeon then finds and removes the tumor, or as much of the tumor as possible without risk of severe damage to the brain. The translabyrinthine procedure provides the best approach for removal of acoustic neuromas when the patient has no useful hearing or hearing function to sacrifice. Complete hearing loss occurs as a result of the removal of the semicircular canals.
- Orbitozygomatic Craniotomy
This refers to a traditional skull base approach used to target difficult tumors and aneurysms. It provides the concept that removal of extra bone proves safer than to unnecessarily manipulate the brain. Brain tumors treated with orbitozygomatic craniotomy include craniopharyngiomas, pituitary tumors, and meningiomas.
Other types of craniotomy include:
- Minimally invasive supra-orbital “eyebrow” craniotomy
- Extended bifrontal craniotomy
Reasons for Stereotactic Craniotomy
A patient may require stereotactic craniotomy for a variety of reasons, including, but not limited to, the following:
- Clipping or repair of an aneurysm
- Removal of an arteriovenous malformation (AVM) or addressing an arteriovenous fistula(AVF)
- Repairing skull fractures
- Treating epilepsy
- Implanting stimulator devices to treat movement disorders such as Parkinson’s disease or dystonia
- Relieving pressure within the brain (intracranial pressure) by removing damaged or swollen areas of the brain that may have occurred due to traumatic injury or stroke
- Diagnosing, removing, or treating brain tumors
What’s the Risks Associated with Stereotactic Craniotomy?
Stereotactic craniotomy involves a highly complex surgery. Complications of this procedure may include:
- Headache
- Infection
- Seizures
- Damage to cranial nerves, the nerves supplying the head and neck region
- Diabetes insipidus due to damage to the pituitary gland, an important endocrine gland in the brain
- Leakage of cerebrospinal fluid (CSF), the fluid surrounding the brain, through the cut area if not closed properly
- Bleeding resulting in the formation of a hematoma. The patient may require a repeat surgery to remove the hematoma
- Air embolism, where air enters a blood vessel and interferes with blood supply to a particular region. Insertion of a CVP line (central venous pressure line) just before the surgery helps to remove any possible air embolisms.