ERECTOR SPINAE PLANE BLOCK
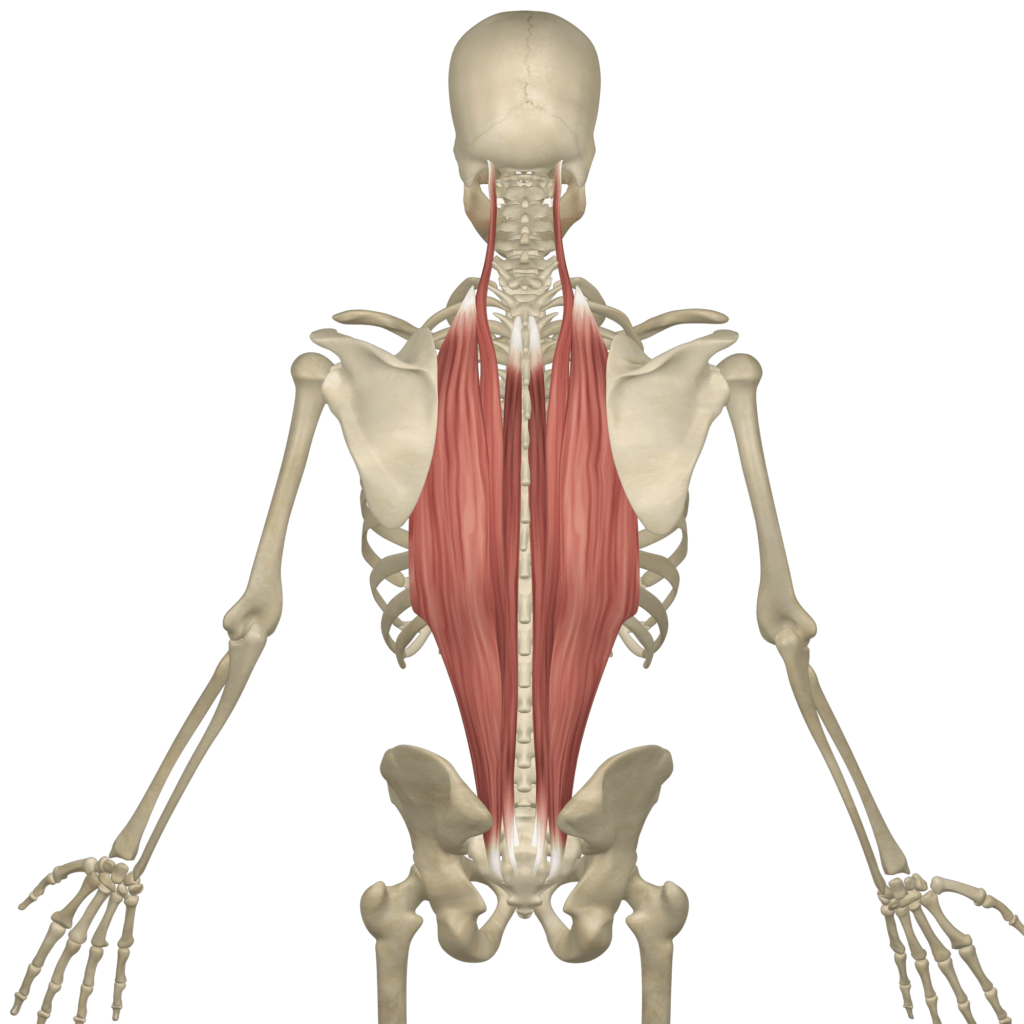
Before understanding the concept of Erector Spinae Plane Block, one must first have comprehensive knowledge of the erector spinae. The erector spinae refer to three indermediate intrinsic muscles of the back- the iliocostalis, longissimus and spinalis. Together, these muscles form a column, known as the erector spinae. These muscles lay posterolaterally to the spinal column, between the spinous processes of the vertebrae and the costal angle of the ribs.
What’s Erector Spinae Plane Block?
The erector spinae plane (ESP) block refers to a new interfascial technique used to provide analgesia (loss of pain sensation) for chronic pain in the thoracic region. It consists of an injection of local anesthetic in a plane between the erector spinae muscles and the transverse processes of the vertebrae. This plane refers to the erector spinae plane. ESP block requires certain medical personnel; an anesthesiologist with knowledge and experience in regional anesthesia, A nurse or physician for assistance. Equipment required for this procedure includes;
- An antiseptic/disinfectant used for skin disinfection before surgery and sterilization of surgical instruments, such as chlorhexidine gluconate
- Sterile gloves, hair cover, mask
- A convex or curved linear probe, used for thoraco-abdominal scans
- ESP block local anesthetic solution (preferably 0.25% bupivacaine or 0.5% ropivacaine 20 to 30ml)
- Standard epidural catheter tray with a 3ml syringe with lidocaine 1% on a 25-gauge needle, 18-gauge Tuohy needle, and an epidural catheter (in the case of continuous infusion)
Methods of ESP Block
The procedure involves two methods; superficial needle or deep needle method.
In superficial needle approach, the specialist injects a drug between the rhomboid major muscle and erector spinae muscle. This technique comes with numerous applications. Its applications range from control of acute postoperative pain to chronic pain.
The deep needle approach presents as a more recommendable method during injection of a drug closer to the costotransverse foramina and origin of dorsal and ventral rami. This approach proves to have effect at the origin of the spinal nerves, based on cadaveric and contrast research.
After the injection of dye into the interfascial plane deep to erector spinae muscle bilaterally, observations showed craniocaudal spread of the dye from C7 to T8 on the right side. From T1 to T8 on the left side, the same occurred in the paraspinous gutter with lateral spread to the transverse processes at all levels. Studies also showed the dye spread slightly beyond the costotransverse junctions at T3 to T6 vertebral levels on the right and T4 to T8 on the left. Cadaveric studies have also shown that a block at T5 level proves sufficient to have unilateral multidermatomal sensory block extending from T1 to L3. This block serves the purpose of a paravertebral block without risk of injury to the pleura.
Before Initiating the procedure, one must acquire consent from the patient, informing the patient on the benefits of this procedure, as well as the possible complications. Also, the anesthesiologist must confirm certain parameters, such as the type of procedure, side, location of the procedure and ensure the absence of complications.
Medical personnel must follow patient monitoring measures such as blood pressure measurement, continuous monitoring of ECG and oxygen saturation (pulse oximetry). Normal level of oxygen usually ranges from 95% or higher. Patients should have prepping performed with chlorhexidine gluconate and sterile conditions maintained throughout the duration of the procedure.
Complications
Post-operation, ruling out certain complications should come into consideration. Complications may prove rare, because of the distance between the site of injection and the pleura, major blood vessels and the spinal cord. The primary complications may include infection at the site of needle insertion, pleural puncture, pneumothorax, toxicity or allergic reactions to local anesthetic, and vascular puncture. However, because of little publicized data, carrying out more research will prove instrumental to gaining better understanding of the safety, complication rates, and effectiveness of this procedure.
Clinical Importance
ESP block has proven use by anesthesiologists to provide loss of pain sensation for a variety of conditions ranging from chronic back ache to pain following hip surgery. Continuous ESP research has commenced to determine if ESP blocks lead to a significant decline in opioid consumption, lower body pain and duration of hospital stay.
References
- Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg Anesth Pain Med. 2016 Sep-Oct.
- https://www.ncbi.nlm.nih.gov/books/NBK54305/
- https://emedicine.medscape.com/article/2116433-overview