CRANIOTOMY
What’s a Craniotomy?
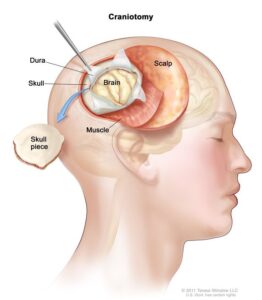
The surgical term “Craniotomy” commonly refers to a type of brain surgery (Stevanovic, Rossaint, Veldeman, & Bilotta, 2016). This operation involves the temporary removal of the bone flap from the skull to expose the brain. In general, a neurosurgeon performs this operation to remove brain tumors and aneurysms. During this operation, neurosurgeons require specialized tools to remove the portion of the bone temporarily. Later, they replace the bone along with tiny titanium plates and screws at the end of the procedure.
Conditions for Craniotomy
Neurosurgeons perform a craniotomy as a life-saving surgery for patients with brain lesions, tumors, hydrocephalus, blood clots (hematoma), foreign body removals such as bullets, or traumatic brain damage (TBI). Also, this operation allows the neurosurgeons to implant surgical devices such as deep brain stimulators to treat Parkinson’s disease, cerebellar tremors, and epilepsy. In epilepsy surgery, neurosurgeons use this technique to remove the portions of the brain that cause seizures. Other reasons for performing a craniotomy may include (Horsfall et al., 2020):
- Removal of arteriovenous malformation (AVM)
- Draining an abscess
- Repairing or clipping a cerebral aneurysm.
- Repairing a skull fracture
- Repairing the covering of the brain, known as dura mater
- Removal of an epileptogenic lesion
- Reducing intracranial pressure by removing damaged or bulging parts of the brain
- Performing microvascular decompression surgery
Different Types of Craniotomy
The type of craniotomy depends on various factors, such as the location and size of the operation. Fort Worth Neurosurgeon names a craniotomy based on the involvement of bone during operation such as occipital craniotomy, parietal craniotomy, frontal craniotomy, temporal craniotomy, etc. The most common craniotomies include (Zhang & Gelb, 2018):
- Pterional Craniotomy
This involves a tiny incision at the intersection of four bones within the skull (frontal, temporal, sphenoid, and parietal) to access and remove a tumor.
- Eyebrow Craniotomy
This involves an incision within the eyebrow to access tumors in the front of the brain, i.e. Rathke’s cleft cysts, pituitary tumors, and skull base tumors.
- Keyhole Craniotomy
This includes removing lesions deep inside the brain, such as meningioma, brain tumors, and acoustic neuroma, through a tiny hole behind the ear.
- Orbito-zygomatic Craniotomy
This involves creating an incision in the scalp beneath the hairline and removing the bone that creates the shape of the orbit and cheek to remove tumors and aneurysms.
- Trans-labyrinthine Craniotomy
This helps to remove the mastoid and some part of the inner ear bone by creating an incision in the scalp behind the ear.
- Awake craniotomy
Neurosurgeons perform this type of craniotomy during the epileptic surgery by awaking the patient to access their response.
This craniotomy involves the use of 3-dimensional imaging techniques such as MRI or CT-scan to detect the treatment location.
Risks of a Craniotomy
Complications can occur during any operation. The incidence of bacterial meningitis or viral meningitis after craniotomy operation ranges from 0.8 to 1.5% (Jiménez-Martínez et al., 2019). According to the Journal of Neurosurgery, risk factors for a craniotomy include early age, long duration of operation, use of steroids, antibiotic prophylaxis, etc.
Craniotomies can result in some possible complications such as infections in the surgical site, excessive blood loss, blood clot, leakage of cerebrospinal fluid, cerebral infarct, memory problems, speech difficulty, unstable blood pressure, subdural empyema, extradural abscess, neurological impairments such as seizures, paralysis, or even coma. In the USA, insured patients reported a postoperative death rate of 1.3 percent and 2.6 percent in uninsured patients after surgery for brain tumors (Gouello et al., 2014).
How Should a Patient Prepare For a Craniotomy Procedure?
Before the surgery, neurosurgeons will explain the risk and benefits of having surgery and take a brief medical history of the patient. Patients need to sign the consent form before the surgery. Later, physicians will perform various presurgical tests such as blood tests, electrocardiograms, chest X-rays, etc. to determine the condition of the patient. Patients need to avoid taking non-steroidal anti-inflammatory medicines (ibuprofen, naproxen, etc.) and blood thinners (Coumadin, aspirin, Plavix, etc.) 7 days before surgery.
How Does a Neurosurgeon perform a Craniotomy?
Craniotomies require a professional medical team lead by a neurosurgeon to successfully perform. During the procedure:
- The patient will lie on the operation table and the anesthesiologists will administer general anesthesia to help them fall asleep throughout the operation.
- Neurosurgeons will make a 1/4-inch skin incision in the targeted area of head.
- After lifting and folding the skin and muscles, the neurosurgeon will drill the skull to make a burr hole. This will ultimately help the neurosurgeon to expose the brain.
- Later, neurosurgeons will correct the problems inside the brain and reattach the bone flap using plates, sutures, or wires.
- The neurosurgeon will suture the skin incision back together to end the operation.
What to Expect From a Craniotomy Recovery?
The length of time to recuperate from a craniotomy varies from person to person. Nurses need to check every patient’s vital signs after they awaken from anesthesia. Following surgery, each patient needs to attend follow-up visits for 10 to 14 days. Depending on the patient’s health, recovery might take anywhere from one to four weeks. It may take up to 8 weeks for the patient to fully recover. For any post-operative questions or concerns, please contact us.
If You need of a Fort Worth Neurosurgeon, Contact Longhorn Brain & Spine Immediately To Get a Consultation.
References
Gouello, G., Hamel, O., Asehnoune, K., Bord, E., Robert, R., & Buffenoir, K. (2014). Study of the Long-Term Results of Decompressive Craniectomy after Severe Traumatic Brain Injury Based on a Series of 60 Consecutive Cases. 2014.
Horsfall, H. L., Mohan, M., Devi, B. I., Adeleye, A. O., Shukla, D. P., Bhat, D., … Khan, T. (2020). Hinge / floating craniotomy as an alternative technique for cerebral decompression : a scoping review. 1493–1507.
Jiménez-Martínez, E., Cuervo, G., Hornero, A., Ciercoles, P., Gabarrós, A., Cabellos, C., … Pujol, M. (2019). Risk factors for surgical site infection after craniotomy: A prospective cohort study. Antimicrobial Resistance and Infection Control, 8(1), 4–11. https://doi.org/10.1186/s13756-019-0525-3
Stevanovic, A., Rossaint, R., Veldeman, M., & Bilotta, F. (2016). Anaesthesia Management for Awake Craniotomy : Systematic Review and Meta- Analysis. 12–23. https://doi.org/10.1371/journal.pone.0156448
Zhang, K., & Gelb, A. W. (2018). Colombian Journal of Anesthesiology Awake craniotomy : indications , bene fi ts , and techniques Craneotomía en el paciente despierto : Indicaciones ,. 46, 46–51.